 I met a lovely 53 year old gentleman, who was suffering from severe low back and hip pain for over a year, diagnosed with a herniated disc. He had tried physical therapy with some relief, but still was unable to eliminate his pain. After diagnosing and treating muscles in his low back, buttock, and thigh, he reported no low back pain, and was discharged from our office. However, after five years, he returned to our office, stating that he had foot pain, diagnosed with plantar fasciitis, and unable to rock climb or hike without severe pain in his calves and feet. After identifying and treating multiple muscles in his calves, shins, and feet, he reported 100% relief, and even finished a 10 day rock climbing trip. Although you may be given one diagnosis, sometimes we find muscle involvement and are able to eliminate the pain!
I met a lovely 53 year old gentleman, who was suffering from severe low back and hip pain for over a year, diagnosed with a herniated disc. He had tried physical therapy with some relief, but still was unable to eliminate his pain. After diagnosing and treating muscles in his low back, buttock, and thigh, he reported no low back pain, and was discharged from our office. However, after five years, he returned to our office, stating that he had foot pain, diagnosed with plantar fasciitis, and unable to rock climb or hike without severe pain in his calves and feet. After identifying and treating multiple muscles in his calves, shins, and feet, he reported 100% relief, and even finished a 10 day rock climbing trip. Although you may be given one diagnosis, sometimes we find muscle involvement and are able to eliminate the pain!
Archive for 'back pain relief'
How important is your diagnosis?

The Start of Baseball Season
The baseball season just opened and already players are calling off their first few games due to “tweaked knees” and “sore backs”. As the sun is starting to come out, and the snow is (FINALLY!) melting, many of us are anxious to get outside and start playing sports again. However, this is also a time where pain can start rearing its ugly head. Many people forget to limber and stretch properly before AND after playing sports, causing strains and sprains of muscles.
So keep in mind these important tips to get moving again this spring:
- Do gentle limbering stretches every day to help maintain flexibility of your muscles.
- Stretch before and after any exercise.
- Start slowly – if you haven’t moved all winter, start with simple exercises, like walking, before starting anything more difficult.
- If you’re feeling extremely sore the following day, it means you may have done too much. Cut back on the difficulty and amount of time the next time you exercise. Slowly increase the difficulty and the length of the session. A safe rule of thumb is to start out after a long layoff at 50% of your prior routine and then increase 15-20% every 5-7 days as long as you feel okay at any level before going to the next.
- Drink lots of water!
Smoking and Back Pain – is it related?
We all know that smoking is bad for you. In fact, since 1965, the Surgeon General’s Warning posted on every package of cigarettes says: Smoking Causes Lung Cancer, Heart Disease, Emphysema, And May Complicate Pregnancy. But did you know that in addition to the myriad of illnesses that are related to tobacco and smoking, recent studies show that smokers have a higher prevalence of back pain than non-smokers? It’s true.
Several studies in the 1980s and 1990s have shown a correlation between smoking and increased back pain. More recently, a  meta-analysis was done in 2010, which basically means a large number of studies (in this case, 40) were put together, and the results were compared to see what pattern, if any, existed between back pain and smoking. This meta-analysis concluded that current and former smokers have a higher prevalence of back pain. It even made the comparison between adult smokers to adolescent smokers; adolescents showed a higher prevalence of back pain. Therefore, we can conclude, the earlier one smokes, the greater risk to your back.
meta-analysis was done in 2010, which basically means a large number of studies (in this case, 40) were put together, and the results were compared to see what pattern, if any, existed between back pain and smoking. This meta-analysis concluded that current and former smokers have a higher prevalence of back pain. It even made the comparison between adult smokers to adolescent smokers; adolescents showed a higher prevalence of back pain. Therefore, we can conclude, the earlier one smokes, the greater risk to your back.
Is there a technical or medical reason behind this connection? Indeed. Smoking causes constriction of blood vessels, which reduces the amount of blood going to your muscles. Decreased blood results in decreased oxygen, which is one of the most important factors in initiating muscle pain. Some smokers actually had parts of their arms and legs amputated because of dead tissue caused by too little oxygen.
Do you want be free of back pain? Put out that cigarette and quit smoking!
When Making Medical Decisions About Pain Relief, Is More Information Better?
In today’s world we are bombarded by information and ways to obtain it. Do you want to know how many steps you take a day? Just buy a device and it will calculate it for you. Care to know what your cholesterol levels are? Simply go get a kit at your nearest drug store. Is it possible we are gathering too much information for our own good?
The same question can be asked about medical testing. Is it useful or even helpful to know certain things about our bodies? Many of us have undoubtedly had the experience where we have gone to the doctor because we had pain and an imaging study was ordered. MRI, CT, and ultrasound can give us information about our bodies that would have been unimaginable in the past.
While technology in general is of course a huge benefit, at the Norman Marcus Pain Institute, we believe it is necessary to proceed with caution as we navigate through it all. At NMPI, one common problem we find in back pain, neck pain, and shoulder pain is the overuse and overreliance on imaging studies. “Abnormalities” are often found on imaging studies without any relation to one’s pain. In fact, seeing abnormalities is more common than seeing a “normal” spine! For example, up to 40% of people without back pain can have herniated discs and as many as 70% may have degenerated discs. That is why the US Institute of Medicine suggests not getting an MRI too quickly since you are likely to see one of these problems and assume it is the cause of your pain. This can lead to unnecessary nerve blocks and surgery.
herniated discs and as many as 70% may have degenerated discs. That is why the US Institute of Medicine suggests not getting an MRI too quickly since you are likely to see one of these problems and assume it is the cause of your pain. This can lead to unnecessary nerve blocks and surgery.
At NMPI, we often see patients who have a herniated disc, yet they only have pain in their back and buttock. They have not experienced any radiation into the leg(s) at all. In these patients, the pain generally has nothing to do with the disc herniation since disc herniation pain generally radiates down the leg and into the foot. Even when the patient is experiencing pain down the leg with a herniated disc found on MRI, muscles in the low back and buttocks may be the cause of the pain. If muscles are not examined as a potential cause, you may undergo an apparently reasonable surgery, without achieving relief of pain. Some studies show that up to 50% of spine surgeries fail (resulting in failed back surgery syndrome) and one of the reasons is the failure to identify muscles that were the true source of the pain.
Most back pain and neck pain is caused by soft tissue such as muscles and tendons. This is confusing because you may have been told your pain is from your spine, discs, or nerves. The problem is most people as they get older have signs of wear and tear on their x-rays and MRIs, but these common signs of aging may not explain your pain if the pain actually originates in your muscles. That’s why we say, when diagnosing persistent pain it’s not having “more” information at hand, it’s having the “right” information at hand.
At NMPI, we often see patients who experience persistent pain even after multiple spine surgeries. Our non-surgical, non-invasive treatment program has most of our patients leaving our office free of long standing back, neck, shoulder, and headache pain.
Is Looking Good Worth Having Back Pain?
There is an old expression, “beauty is pain.” Does it need to be? Is it worth risking your long-term health? Why do women wear high-heeled shoes when they know that looking beautiful in the moment may cause them pain down the road? Scientists from the Universite de Bretagne-Sud recently conducted experiments, which studied the effects of high-heeled women on men. Women who wore higher heels (3-4 inches vs. 2 inch heels) were able to get more men to answer survey questions on the streets and were picked up faster in bars and clubs. These studies show some type of empowerment in women with high-heeled shoes.  Knowing that this empowerment exists, and as fashion has increased the height of heels from 4 inches to 5 inches, we would like to remind you that walking for extended periods in high heels can cause calf tendons to shorten and possibly result in an increase in low back pain.
Knowing that this empowerment exists, and as fashion has increased the height of heels from 4 inches to 5 inches, we would like to remind you that walking for extended periods in high heels can cause calf tendons to shorten and possibly result in an increase in low back pain.
Here at the Norman Marcus Pain Institute, we see patients that run the gamut of factors causing their back pain. Prevention is always the best treatment; since low back pain affects so many of us a simple intervention is being more conscious of our shoes! While those Manolo Blahniks and Jimmy Choos may be stunning, they may be causing a problem for you down the line. At NMPI, we won’t say don’t wear them, just please, wear them in moderation.
Men, Women, and Children — Simple Solutions to Eliminate Back Pain
Men:
Where do you keep your wallet? Many of you probably answered, “your back pocket.” Did you know that this could be causing your back pain?
When you sit down with your wallet in your back pocket, it presses into your muscles, which can cause pain in your low back and buttock. The squeezed muscle can press your sciatic nerve causing the pain to travel down your leg.
If you’re suffering from back pain, try keeping your wallet in an external bag or a front pocket. Or simply decrease the thickness of your wallet by taking out any extraneous items, such as old receipts or credit cards that you no longer need or use.
Women:
Those fashionable Jimmy Choos or Manolo Blahnik’s, which are known for their height, may actually be increasing your low back pain. But don’t switch out those high heels for the increasingly popular ballet flats or stylish sandals because flats can stretch and strain the muscles in the calves and thighs causing pain in the buttock and low back.
You don’t have to forgo fashion for comfort. Wearing low, comfortable heels can save your back from unnecessary pain. Remember to wear shoes that fit properly as well – ill-fitting shoes can cause you to tighten your leg and buttock muscles causing low back, buttock, and leg pain.
Children:
Now that school is back in session, many kids are carrying heavy books in their backpacks. Often, the heavy, incorrectly worn backpacks can cause poor posture and strain on muscles. Parents, have your child(ren) pack their backpacks so that the heaviest books are placed towards the back of the bag. This way, the heaviest part of the bag is closer to the back of the child. (see picture) Also, remind your child(ren) to use both straps on both shoulders. This helps distribute the weight evenly, as opposed to placing strain on one shoulder. Another option is using backpacks with rolling capabilities.
Similarly, all you ladies who stuff your shoulder bags with everything from lipstick to workout weights, carrying a heavy bag on your shoulder every day can be the source of your aching neck and back. While those oversize totes conveniently contain everything you might possibly need in a day, the accumulated stress on your neck and spine from “pocketbook overload” can lead to serious strain on your muscles, tendons, nerves, and ligaments, causing serious body aches. So what does a fashionable woman on the go do?
- If you absolutely must carry a tote, lighten the load – try to take out the items you don’t really use or need.
- Switch the bag from one shoulder to the other often, minimizing the amount of time you strain the shoulder and neck muscles.
- Try using two lighter bags instead of one big one. Splitting the load and carrying them on both sides distributes the weight evenly.
And don’t forget; no matter what you carry, having good posture helps reduce back pain.

Parents:
Lifting your baby 50 times per day, or bending and lifting up to get your active toddler out of his/her sibling’s hair, are innocent movements that can indeed cause low back pain. Good posture and proper lifting techniques can help parents avoid the increased risk for low back pain. Some key pointers:
- Keep your feet (shoulder width) apart, your back straight and bend your knees to reach for your child.
- Use your leg muscles, which are bigger and stronger than your back muscles, to lift your child. After you bend over, bring your child to your chest, bring your back to the upright position, and then straighten your legs. If you straighten your legs before bringing your body upright, you’re using your low back muscles to lift your child. However, if you straighten your legs last, then you’re using your leg muscles.
Keep in mind; this is a good tip for lifting anything heavy!
Eating forbidden foods, losing weight and helping your heart
I had dinner with Dr. Robert Atkins years before his untimely death. He ordered a juicy marbleized steak with a baked potato drowning in butter and sour cream. At the time I thought this wasn’t a healthy choice- I was wrong! A front page article in the NY Times earlier this week reports on a large year-long NIH funded study published in the Annals of Internal Medicine supporting the ideas of Dr. Atkins, viz. high fat/ low carbohydrate diets are better for your health than equal calories of high carbohydrate/ low fat diets. You not only lose more weight but your total cholesterol goes down and the good cholesterol (HDLs) goes up. This is a great example of showing us that what we firmly believe to be the truth (i.e. a low fat diet is best for your diet and health) may not be so. An important issue in this study is that both groups lost weight. Calorie restriction does work to lose weight- but it may be easier for some patients who have difficulty dieting, to limit their carbohydrates, still feel satisfied, and lose weight.
 As I report in my book End Back Pain Forever, a previous NIH funded study also showed that calorie reduction consistently resulted in weight loss; this new study reaffirms that low carbohydrate/high fat diets are healthier for your heart. In my book I reported that eating plant rather than animal protein/fat was preferable if you were concerned about lowering levels of the bad cholesterol (low density lipoproteins-LDLs). If you’re thinking of becoming a vegetarian- eating a vegetarian diet has been shown to produce the lowest levels of cholesterol and in general to be associated with the lowest BMIs (Body Mass Index, which is a measure of body fat based on weight and height.). The carbohydrates that are most damaging are refined carbohydrates such as found in white flour and sugar. No matter what diet you choose you need to get the minimal amounts of essential minerals and vitamins, therefore always include healthy amounts of fresh fruits and vegetables.
As I report in my book End Back Pain Forever, a previous NIH funded study also showed that calorie reduction consistently resulted in weight loss; this new study reaffirms that low carbohydrate/high fat diets are healthier for your heart. In my book I reported that eating plant rather than animal protein/fat was preferable if you were concerned about lowering levels of the bad cholesterol (low density lipoproteins-LDLs). If you’re thinking of becoming a vegetarian- eating a vegetarian diet has been shown to produce the lowest levels of cholesterol and in general to be associated with the lowest BMIs (Body Mass Index, which is a measure of body fat based on weight and height.). The carbohydrates that are most damaging are refined carbohydrates such as found in white flour and sugar. No matter what diet you choose you need to get the minimal amounts of essential minerals and vitamins, therefore always include healthy amounts of fresh fruits and vegetables.
To paraphrase Mark Twain, it’s very easy to diet and lose weight- I’ve done it twenty times; The trick is to keep it off once you’ve lost it. Here are some tips from my book:
1. Increase your physical activity. If you never walk anywhere, start to do that. If you walk two blocks a day, increase it to four. If you go to the gym once a week, increase it to twice a week. The idea is to begin where you are now and increase slowly and steadily. Don’t take on more than you can handle, but work your way up. Make yourself a winner by taking on an achievable goal.
2. Don’t attempt total deprivation. Avoid starvation diets. Your body senses that you are starving, and it adjusts by slowing your metabolism, the rate at which calories are burned. This makes it harder to lose weight. Being able to lose weight and maintain the loss requires changing the way you eat and increasing physical activity. Just as you changed your activity level gradually, do the same with diet. In other words, start slowly. Make one simple change. I recommend to my patients that they stop eating bread and pastries. Some love bread and can’t imagine living without it. They soon learn, though, that after a short while, the craving for bread diminishes and their weight starts to drop. Then stop eating pasta or only allow it (and bread) as a treat; let’s say on Sundays.
3. Learn how many calories are in the food that you eat. When patients tell me that all they eat is salad, but they’re gaining weight, I have to remind them that any sauce or dressing may contain high-calorie ingredients. When you are out at a restaurant, it is best to avoid foods that may hide unwanted calories.
Is Bad Weather To Blame For Your Lower Back Pain?
A New York Times article Weather May Not Affect Back Pain, printed mid-July, cited a study showing that weather may not affect back pain. The purpose of the study was to explore the often-heard complaint from patients diagnosed with persistent pain related to muscles and bones (musculoskeletal pain) that weather changes cause an increase in pain. The study was based on an analysis of 993 patients who had seen their physician in 2011-2012 complaining of an episode of sudden back pain. These were not patients with a history of back pain.
So this article does not actually examine patients who already have back pain to see if the pain is increased with bad weather. In my practice, at NMPI, I have patients who can tell me a snowstorm is coming 3 days before it occurs. Although studies of the association between weather and pain are not uniformly supportive of the connection, a study done in 1995 of 558 patients with chronic pain found that 2/3 experienced an increase in pain and most of them prior to the occurrence of the bad weather.
 I have patients whose pain is so severe with bad weather that they can hardly get out of bed. Although there is no good scientific explanation for this association, some suggestions have been offered. When the barometric pressure falls, the air pressure in a painful joint may continue to be a little higher than the air pressure on the outside of the body, causing an increase in pain. Another explanation is that cold and/or inclement weather decreases the amount of time you are outside and active. Patients with musculoskeletal problems (i.e. muscle pain and arthritis) often feel worse with inactivity. In addition cold weather causes the blood vessels in the hands and feet to constrict, which can decrease the amount of available oxygen, resulting in increased muscle pain.
I have patients whose pain is so severe with bad weather that they can hardly get out of bed. Although there is no good scientific explanation for this association, some suggestions have been offered. When the barometric pressure falls, the air pressure in a painful joint may continue to be a little higher than the air pressure on the outside of the body, causing an increase in pain. Another explanation is that cold and/or inclement weather decreases the amount of time you are outside and active. Patients with musculoskeletal problems (i.e. muscle pain and arthritis) often feel worse with inactivity. In addition cold weather causes the blood vessels in the hands and feet to constrict, which can decrease the amount of available oxygen, resulting in increased muscle pain.
If your history indicates that bad weather causes an increase in your pain, it is likely that your flare up is most likely not an indicator of physical deterioration. Additional pain can be reasonably treated with increased medication for the brief period of weather related pain.
Epidural steroids are not effective for spinal stenosis
I have been suggesting for many years that there is an overuse of spinal injections and surgeries for low back and leg pain, so it was no surprise when I read an article in The New York Times (NYT) that reported on a study recently published in the New England Journal of Medicine[1] about patients with spinal stenosis who are frequently treated with a procedure that has been shown to be ineffective. Epidural steroid and lidocaine injections for patients found to have spinal stenosis were no better than epidural injections of lidocaine alone. In chapter 4 of my book End Back Pain Forever I discuss the many reasons for back pain. MRIs and CT scans of the low back will almost always find something such as spinal stenosis or a degenerated or herniated disc even in patients without pain. Therefore the US Institute of Medicine suggests that these imaging studies should not be done routinely since what you find in the study is frequently not the cause of your pain. The most common cause of back pain is muscles and other soft tissue. If you treat the diagnosis you got from the MRI or CT and the actual reason for the pain is muscle, it makes sense that the treatment will frequently fail, which it does!
The NYT report of this relatively large, randomized, double blind, controlled study clearly demonstrates the ineffectiveness of the use of steroids for symptoms attributable to spinal stenosis (narrowing of the canal in the spine which contains the spinal cord) which occurs frequently as we age. The treatments most often provided are epidural steroids to theoretically reduce the inflammation of the nerves being squeezed by the narrow canal, and surgery to widen the canal. Both approaches have a significant failure rate.
At the Norman Marcus Pain Institute we have shown in multiple published articles that one reason why these approaches are ineffective is that the pain in the back and leg may not be the result of the narrowing or other supposed abnormalities seen on the MRI or CT scan. It is well known that very few (in one published article- less than 10%) scans of the low back in adults are read as normal; as many as 40% of adults with no back pain have herniated discs, and 70% have degenerated discs. So it is “normal” to find an abnormality.
Our unique physical examination, utilizes an instrument I developed, reveals that many patients with back and leg pains have areas of muscle tenderness that are the source of their pain yet are overlooked. One study of more than 23,000 patients[2] found that 70-80% of patients with back pain were diagnosed with sprains and strains of muscle and other soft tissue. It’s hard to believe then, armed with this knowledge, that muscle examination and treatment is not part of the typical standard of care for back pain in the USA[3]. If we are to properly address the cause of most back pain, the evaluation and treatment of its muscular causes must be addressed.
[1] Friedly JL, Comstock BA, Turner JA, et al. A Randomized Trial of Epidural Glucocorticoid Injections for Spinal Stenosis. New England Journal of Medicine. 2014:374:11-21.
[2] Deyo RA, Weinstein JN. Primary care – low back pain. New England Journal of Medicine. 2001:5:363-70.
[3] Chou R, Qaseem A, Snow V, Casey D, Cross JT, Shekelle P, et al. Diagnosis and Treatment of Low Back Pain: A Joint Clinical Practice Guideline from the American College of Physicians and the American Pain Society. Ann Intern Med. 2007;147:478-491.
Stiffness is an important aspect of muscle pain
I recently saw George, a 48-year-old man, who suffered from pain, described as soreness in the thighs, neck, shoulders and arms, and tingling in his calves and shin. Sitting for more than two hours or sitting for more than 20 minutes would cause an increase in his pain. Bending over also brought on his pain.
George had tried physical therapy on multiple occasions, and saw two neurologists, who could not find anything that would explain his pain.
When I examined him, I found him to be strong but very stiff. When he bent over, he was able to reach within 14 inches of the floor. When he lied on his back and lifted one leg up at a time, he was able to reach only 57 degrees (85 75 degrees is normal). Because he was so stiff, I decided to start a course of exercises that would help increase his range of motion.
Over the next few weeks, George learned all 21 of the Kraus-Marcus exercises, which he was advised to do every day. As he did the exercises, he noticed that his pain level was decreasing and wasn’t occurring as often as usual. When he was taught the last 7 exercises, he was able to bend over to within 9 inches of the floor, and could lift each leg to 80 degrees.
A month later, George reports a 90% decrease in his overall pain. Sometimes we find that starting with the most conservative of treatments can prevent us from performing more costly and dangerous treatments. Very often, stiffness is an important aspect of one’s pain that can easily be found and treated!
Low Level Laser Therapy as promising treatment
Low level laser therapy (LLLT) is a promising new treatment for a variety of painful conditions which is believed to reduce inflammation and stimulate healing of wounds. Interest in the laser first developed when Endre Mester at Semmelweis University noticed that applying the laser to the backs of shaven mice caused hair to regrow faster than those who did not receive laser treatment.[1] This observation prompted further study into the regenerative effects of the laser first in rats, and then later in humans.
Currently, there aren’t many large-scale studies evaluating the effectiveness of the laser, but smaller studies of the laser for painful conditions show promising results.
A study of 50 patients with knee osteoarthritis reported that the laser was significantly more effective at providing pain relief than transcutaneous electric nerve stimulation (TENS)**.[2] Similarly, a separate study of 125 patients with knee osteoarthritis reported both an improvement in pain and an increase in function after LLLT.[3]
In a study of patients with temporomandibular disorders, the laser improved pain within 24 hours, with relief lasting at the 180 day follow-up.[4]
Current studies show that the laser is an up and coming, non-invasive, non-painful treatment option, but larger studies are needed to determine the correct dosing, and for which conditions the laser will be most useful.
**TENS (transcutaneous electrical stimulation) – electrodes are applied to the skin, sending an electric current to the nerves in the skin. The nerves then transmit a signal to the brain. This signal is competing with the signal coming from your painful area. So, instead of feeling your normal pain, you’ll feel a buzzing sensation where the electrodes are attached.
[1] Chung, Hoon, Tianhong Dai, Sulbha K. Sharma, Ying-Ying Huang, James D. Carroll, and Michael R. Hamblin. “The Nuts and Bolts of Low-level Laser (Light) Therapy.” Annals of Biomedical Engineering 40.2 (2012): 516-33. Print.
[2] Kędzierski, Tomasz, Katarzyna Stańczak, Kamila Gworys, Jowita Gasztych, Marcin Sibiński, and Jolanta Kujawa. “Comparative Evaluation of the Direct Analgesic Efficacy of Selected Physiotherapeutic Methods in Subjects with Knee Joint Degenerative Disease – Preliminary Report.” Ortopedia Traumatologia Rehabilitacja 14.6 (2012): 1-10. Print.
[3] Gworys, Kamila, Jowita Gasztych, Anna Puzder, Przemysław Gworys, and Jolanta Kujawa. “Influence of Various Laser Therapy Methods on Knee Joint Pain and Function in Patients with Knee Osteoarthritis.” Ortopedia Traumatologia Rehabilitacja 14.3 (2012): 269-77. Print.
[4] Pereira, T. S., O. D. Flecha, R. C. Guimaraes, A. M. Botelho, JC Ramos Gloria, and K. T. Aguiar Tavano. “Efficacy of Red and Infrared Lasers in Treatment of Temporomandibular Disorders–a Double-blind, Randomized, Parallel Clinical Trial.” Cranio : The Journal of Craniomandibular Practice 32.1 (2014): n. pag. Ovid. Web.
NSAIDs for pain relief
The next series of blogs is a brief discussion of different types of medications used for pain.
NSAIDs
Non-steroidal anti-inflammatory drugs (NSAIDs) are generally one of the first line of medications used in the initial treatment of pain. They are exactly what their name means – they are not steroid medications (like cortisone or prednisone) and they reduce inflammation which is the body’s response to any damage from any cause. When inflammation occurs there is pain along with redness, swelling and heat, which are collectively known as the cardinal signs of inflammation. Examples of NSAIDs are ibuprofen (Advil/Motrin), naproxen (Naprosyn), meloxicam (Mobic), and diclofenac (Voltaren). Aspirin is similar to the NSAIDs in almost every way but curiously it helps prevent heart attacks whereas NSAIDs may cause them (see below).
 Although NSAIDs have a number of side effects, the two most common are stomach irritation and an increased tendency to bleed. That’s why you are advised to eat when taking NSAIDs and why you have to stop taking NSAIDS before any type of intervention that may cause bleeding (such as injections or surgery). In order to decrease the side effect of stomach irritation, many have switched to a topical NSAID, most commonly diclofenac which is offered as a patch (Flector-patch) or gel (such as diclofenac or Voltaren gel). Other potentially serious side effects include kidney failure – if your kidneys are not working properly the NSAID can cause them to stop functioning, asthmatic episodes if you are prone to having asthma, and heart attacks if you have cardiovascular disease (heart disease, high blood pressure, history of stroke).
Although NSAIDs have a number of side effects, the two most common are stomach irritation and an increased tendency to bleed. That’s why you are advised to eat when taking NSAIDs and why you have to stop taking NSAIDS before any type of intervention that may cause bleeding (such as injections or surgery). In order to decrease the side effect of stomach irritation, many have switched to a topical NSAID, most commonly diclofenac which is offered as a patch (Flector-patch) or gel (such as diclofenac or Voltaren gel). Other potentially serious side effects include kidney failure – if your kidneys are not working properly the NSAID can cause them to stop functioning, asthmatic episodes if you are prone to having asthma, and heart attacks if you have cardiovascular disease (heart disease, high blood pressure, history of stroke).
Image courtesy of anekoho/FreeDigitalPhotos.net
What are trigger points?
Have you ever felt a painful tightness that just won’t go away no matter how much you stretch? Even if the pain subsides or goes away temporarily, when it recurs you still feel a tender knot that’s always in the same area. This may be due to trigger points (TrPs). TrPs are tender nodules which can cause pain and are found in a taut band of muscle tissue. This taut band is formed from a small group of contracted muscle fibers which will make that region of your muscle feel hard and tender. TrPs are sensitive to pressure and movement. Pressing on a trigger point will cause pain.
TrPs can be classified as either active or latent. A latent TrP is one that causes pain when palpated, or pressed on, but not spontaneously while resting. An active TrP can cause spontaneous pain – either at rest, in use, or while being pressed. If there is enough stress – for example, from too much exercise, a latent TrP can transform into an active TrP.
The cause of TrPs is still being studied, however, there is speculation that the taut band appears in the muscle first without any tenderness or irritation. With additional stress, the hardened area becomes tender to the touch (a latent TrP), and finally, may progress to producing spontaneous pain as an active TrP. The initial hardness in a band of muscle fibers can be caused my multiple factors: injury, overstretching, or over-exercising.
TrPs can be a debilitating source of pain. They can cause weakness and lack of coordination in the muscles where they are found. Next blog, we will discuss common treatment options for trigger points.
Muscles as the source of pain
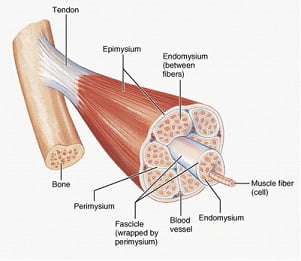
Muscles are the largest organ system in the body, accounting for approximately 50% of our body weight. We have different ways of categorizing muscles: how they look, how they move, and where they’re located. We are going to focus on muscles that move voluntarily, which means we tell the muscles to move, as opposed to involuntary muscles, which automatically move on their own (like our heart and blood vessels). There are 641 muscles in the body – 340 pairs (meaning we have one on the right, and one on the left), and one unpaired (which is the transverse arytenoid for those who must know).
70% of lower back pain is diagnosed as idiopathic or non-specific[1], which means we are not sure what caused the pain. However, most investigators believe that sprains and strains of the soft tissue are the source of pain. Soft tissue refers to muscles, tendons, and ligaments. So it may be surprising that the emphasis in evaluating and treating lower back pain, neck pain, and shoulder pain, is on the spine and the nerves coming out of the spine. In fact, from 1997 to 2005, the prevalence of the diagnosis of spine-related issues has increased 100% while the diagnosis of strains and sprains of soft tissue has gone down by 40%[2].
This is generally attributed to the increase in the use of high-tech imaging studies, such as MRI and CT scans. However, just because we have a clearer image of what’s going on inside of your body doesn’t mean that we have a clearer understanding of what’s causing your pain. More than 90% of lower spine MRIs exams in adults are abnormal[3]. Studies have found that up to 40% of people have herniated discs and as many as 70% have degenerated discs with no pain. If people can walk around with abnormal spines without pain, then this means that abnormalities in the spine aren’t always the cause of pain. Your diagnosis of a herniated disc, spinal stenosis, or spondylosisthesis may actually be unrelated to your source of pain.
Muscles are often ignored when it comes to diagnosing pain. I believe the reason is that we rarely evaluate muscles as a source of pain. We generally don’t learn about or understand how they work, what chemical changes take place inside, and how they produce pain (the pathophysiology). I would like to take the next few blogs to discuss how muscles contribute to your chronic pain.
It is important to understand what any diagnosis means in relationship to your back or leg pain.
I have heard from a number of group members who have been diagnosed with spinal stenosis. The diagnosis is often made based on what is found on a CT scan or MRI without the expected corresponding signs and symptoms. It is important to understand what any diagnosis means in relationship to your back or leg pain.
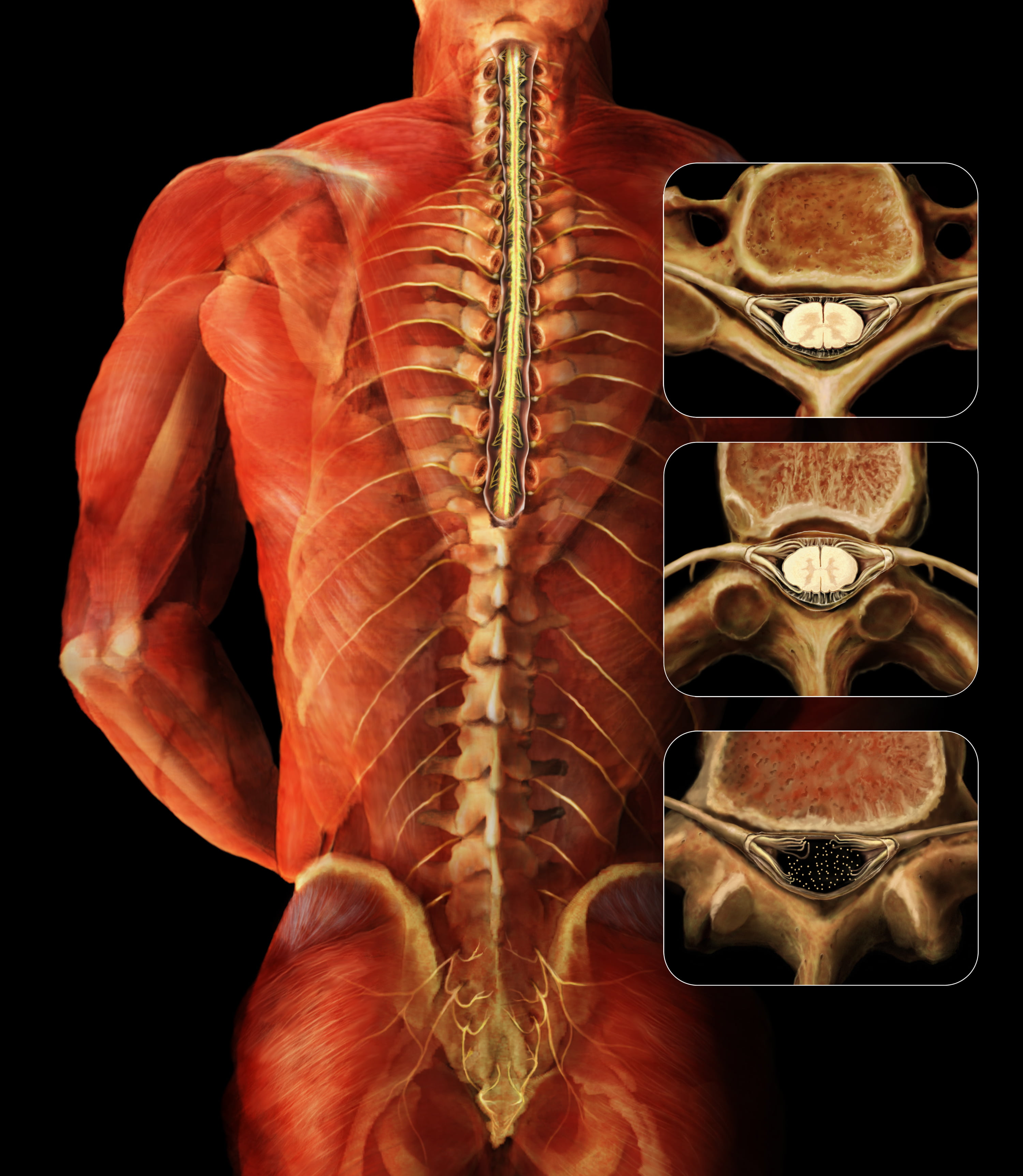
Spinal stenosis is a narrowing of the space formed by the bony segments that together make up the vertebra (the bones of the spine). The space in each vertebra is connected to the vertebra above and below to form the spinal canal, through which the spinal cord passes. Narrowing of the canal in the lumbar region, called lumbar spinal stenosis, could squeeze the spinal cord. When you are standing up, the curve in the spine makes the narrowing worse and may cause pain radiating to the leg. Many patients found to have narrowing don’t have the signs and symptoms that would indicate that their back and leg pain was caused by the narrowing. Bending over when you walk, having more pain if you straighten up, and having to wait a few minutes when you sit down for the pain to go away, are all symptoms that suggest the spinal stenosis was truly the cause of the pain; just finding narrowing with imaging isn’t enough.
Other imaging diagnoses such as degenerative disc disease, degenerative osteoarthritis, bulging or herniated disc, and facet arthropathy, may also be misleading. Just because there is an anatomic finding on an image doesn’t mean it is the cause of the pain. If some form of exercise relieved the pain, the most reasonable explanation would be that much of the pain was related to soft tissue, such as muscle and tendon and not to the imaging diagnoses.
MRI, CT, and X-rays may mistake the cause of your back pain
MRI, CT and X-rays may fool us. A recent article concluded that the amount of constriction of the nerves exiting the lower spine thought to be the reason for back and leg pain was not correlated with the amount of relief a patient experienced with steroid injections around that nerve(s).
Beautiful clear pictures of the spine and nerves seduce us into believing we can see the reason for the pain. Focusing too much on imaging and not enough on the physical examination, results in many patients receiving surgery and nerve blocks that were assumed to be the right treatment but didn’t relieve the pain. Did that happen to you?
Read the rest of this entry
END BACK PAIN FOREVER
by Dr. Norman Marcus

If you or someone you love has been suffering with back pain, this book could change your life.
![]()
